HIPAA Privacy Rule Summary: Requirements And Patient Rights

The HIPAA Privacy Rule governs how protected health information (PHI) moves between healthcare providers, insurers, business associates, and patients. If you're building or operating a healthcare application that touches patient data, especially one that integrates with EHRs, understanding this rule isn't optional. Yet finding a clear HIPAA Privacy Rule summary that cuts through the legal jargon can be surprisingly difficult, and misunderstanding the requirements carries real financial and legal consequences.
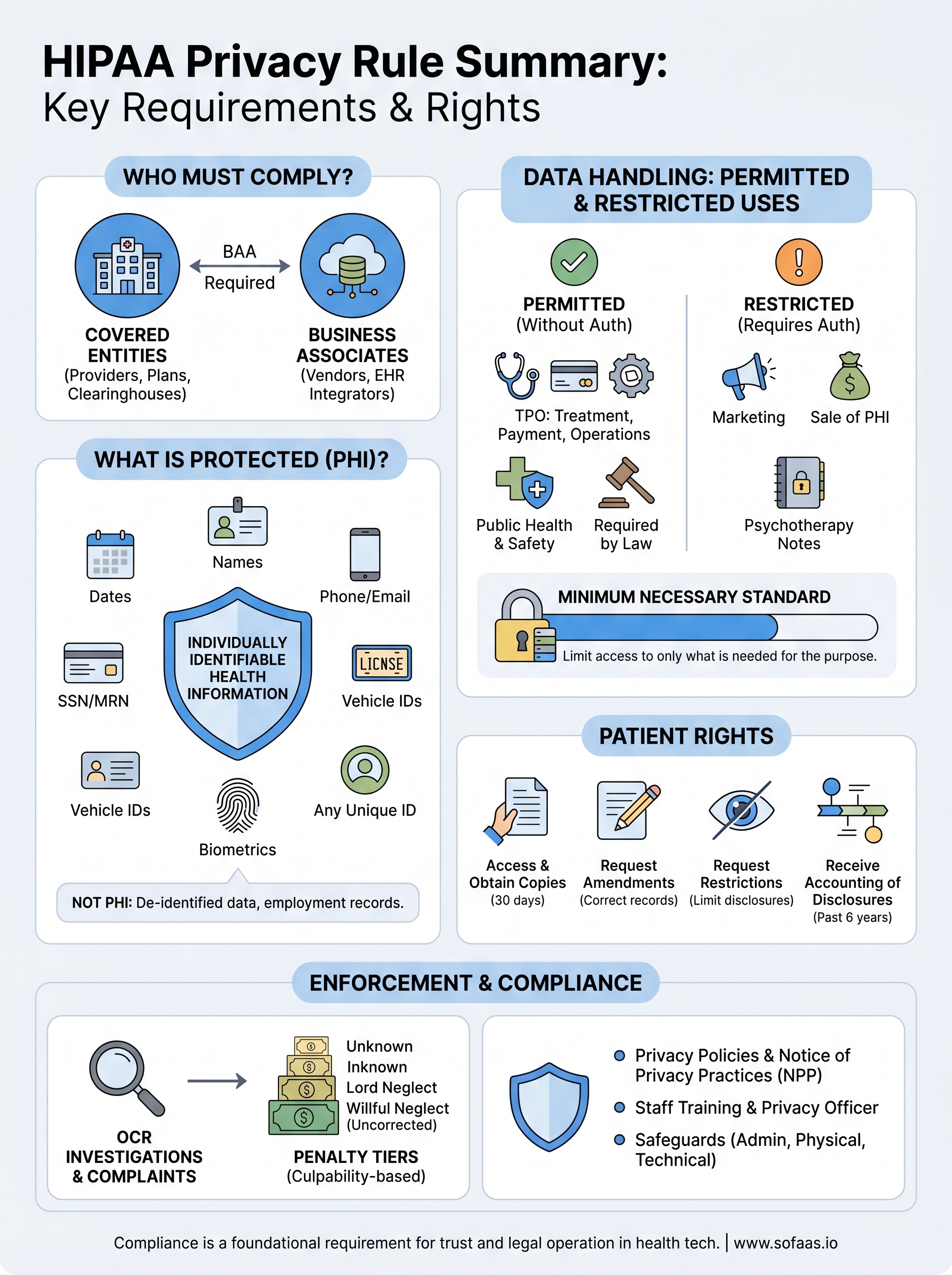
At its core, the Privacy Rule answers four questions: Who must comply? What data is protected? When can that data be used or shared? And what rights do patients have over their own records? These questions matter whether you're a covered entity, a business associate, or a health tech company connecting to Epic, Cerner, or Allscripts through standards like SMART on FHIR. Every data exchange your application handles falls under this rule's reach, making compliance a foundational concern for any integration strategy.
That's exactly why we built SoFaaS, to handle the heavy lifting of HIPAA-compliant healthcare data integration so teams can focus on their applications, not infrastructure and regulatory overhead. But compliance starts with understanding the rules themselves. This article breaks down the HIPAA Privacy Rule into its essential components: covered entities, protected health information, permitted uses and disclosures, patient rights, and enforcement. By the end, you'll have a clear, practical grasp of what the law requires and how it applies to your work.
What the HIPAA Privacy Rule does and does not do
The HIPAA Privacy Rule, formally issued by the U.S. Department of Health and Human Services (HHS) under the Health Insurance Portability and Accountability Act of 1996, sets national standards for protecting identifiable health information. It tells covered entities and their business associates exactly how they can collect, store, use, and disclose protected health information (PHI). Many people treat it as a sweeping, general privacy law, but it has a narrower and more specific scope than that assumption suggests.
What the Privacy Rule actually establishes
The Privacy Rule creates a framework built on two core functions. First, it restricts how PHI can be used and disclosed without a patient's written authorization. Second, it gives patients specific rights over their own health records, including the right to access, amend, and request certain restrictions on how their data is used. Together, these two functions define the boundaries of lawful health data handling for any organization that falls within its scope.
A frequently missed point: the Privacy Rule governs internal uses of PHI as well as external disclosures, meaning your own staff can only access patient data when it is necessary for their specific job function.
Beyond those two pillars, the rule requires covered entities to implement administrative safeguards such as designating a privacy officer, training staff on privacy policies, and maintaining written procedures that accurately reflect actual data practices. This operational layer is a core part of any complete HIPAA privacy rule summary and carries the same legal weight as the disclosure restrictions themselves.
What the Privacy Rule does not do
Understanding the rule's limits is just as important as knowing what it requires, especially for teams building healthcare technology. The rule does not apply to every organization that handles health information. A fitness tracking application, a school health record system, or an employer wellness program generally falls outside its reach because those entities do not qualify as covered entities under HIPAA's specific definitions.
The Privacy Rule also does not prohibit all sharing of PHI. It permits, and in certain cases requires, the exchange of patient data for clearly defined purposes such as treatment coordination, payment processing, and authorized public health activities. The intent is not to lock data away but to ensure that every access point serves a documented, legitimate purpose within an established permission structure.
Finally, the Privacy Rule does not supersede state privacy laws when those laws offer stronger protections. In situations where a state law imposes stricter requirements on health data handling than HIPAA does, the stricter standard takes precedence. For organizations operating across multiple states, this means your effective compliance floor can vary by jurisdiction, and mapping that landscape is a practical requirement before deploying any patient-facing application.
Why the Privacy Rule matters for health data sharing
Health data is fundamentally different from other types of personal information. A compromised credit card number can be replaced in minutes, but a disclosed mental health diagnosis, substance use history, or HIV status can affect someone's employment, insurance, and relationships for years. The Privacy Rule exists because patient data requires a higher standard of protection, and every data flow in your application either respects that standard or puts both patients and your organization at risk.
The rule shapes every integration decision you make
When you build an application that connects to an EHR system, you are not just managing a technical data pipeline. You are operating inside a legally structured information environment where every read, write, and transfer carries compliance implications. Knowing which data fields constitute PHI, which disclosures require patient authorization, and which internal access patterns violate the minimum necessary standard directly determines how you architect your data models, API calls, and access controls.
Getting this wrong does not just create legal exposure. It erodes the patient trust that your entire application depends on.
For health tech teams, a solid HIPAA Privacy Rule summary is not just background reading. It is a design document. The choices you make at the integration layer, from what patient data you request to how long you retain it, all trace back to the rule's requirements. Teams that understand this early avoid expensive redesigns and failed security reviews later.
Trust is the real infrastructure of health data exchange
The healthcare ecosystem runs on information sharing between providers, payers, labs, pharmacies, and patients. Without a consistent legal framework governing how that data moves, the entire system breaks down. The Privacy Rule provides the trust infrastructure that makes it possible for a primary care physician to share records with a specialist, or for your application to pull patient data from Epic on behalf of a consented user, without either party questioning whether that exchange is legitimate.
Your application's ability to access, process, and act on patient data depends on everyone in the chain trusting that the rules are being followed. When you demonstrate that your integration meets Privacy Rule standards, you are not just checking a compliance box. You are proving to health systems, enterprise clients, and patients that your platform belongs in that trusted network.
Who must comply: covered entities and business associates
The HIPAA Privacy Rule does not apply to every organization that handles health data, it applies to specific categories of organizations defined by law. If your company falls into one of those categories, or if you provide services to one, you carry direct legal obligations under the rule. Any complete HIPAA Privacy Rule summary needs to identify these categories clearly, because misclassifying your own organization is one of the most common and costly compliance mistakes in health technology.
Covered entities: the three core categories
The law defines covered entities as the organizations directly regulated by HIPAA, and they fall into three distinct groups. First, healthcare providers that transmit health information electronically in connection with covered transactions, such as billing, are covered. This includes hospitals, physician practices, pharmacies, and clinical labs. Second, health plans including commercial insurers, Medicare, Medicaid, and employer-sponsored group health plans fall under the rule. Third, healthcare clearinghouses that convert non-standard health data into standardized formats are covered entities.

If your application directly bills payers, manages clinical records, or processes health plan data on behalf of any of these organizations, your compliance obligations start here.
Your organization may not qualify as a covered entity itself, but if you build software that processes patient data on behalf of one, you likely fall into the next category, and that distinction carries just as much legal weight.
Business associates and the chain of accountability
A business associate is any person or organization that creates, receives, maintains, or transmits PHI while performing a service for a covered entity. This includes software vendors, cloud storage providers, data analytics firms, billing services, and any platform that processes patient data as part of its core function. If your application connects to an EHR and handles identifiable patient records as part of that integration, you are almost certainly a business associate.
Business associates must sign a Business Associate Agreement (BAA) with each covered entity they serve. The BAA legally binds you to protect PHI in accordance with HIPAA requirements and specifies how your organization can use the data you receive. Covered entities are responsible for obtaining BAAs from all business associates before sharing any PHI, and business associates must secure their own BAAs from any subcontractors that touch that same data.
What counts as PHI and what is not PHI
Knowing exactly where the PHI boundary sits is one of the most practical applications of any HIPAA Privacy Rule summary. Protected health information is not simply any data about a patient's health. The rule defines PHI as individually identifiable health information that is created, received, maintained, or transmitted by a covered entity or business associate. That definition has three components that all need to be present: the data must relate to a person's physical or mental health condition, their healthcare treatment, or their payment for care, and it must be possible to identify the individual from the data.
The 18 identifiers that define PHI
HHS specifies 18 categories of identifiers that, when combined with health information, create PHI under the rule. If your application collects or transmits any of these alongside health data, you are handling PHI and your full compliance obligations apply. The identifiers include:
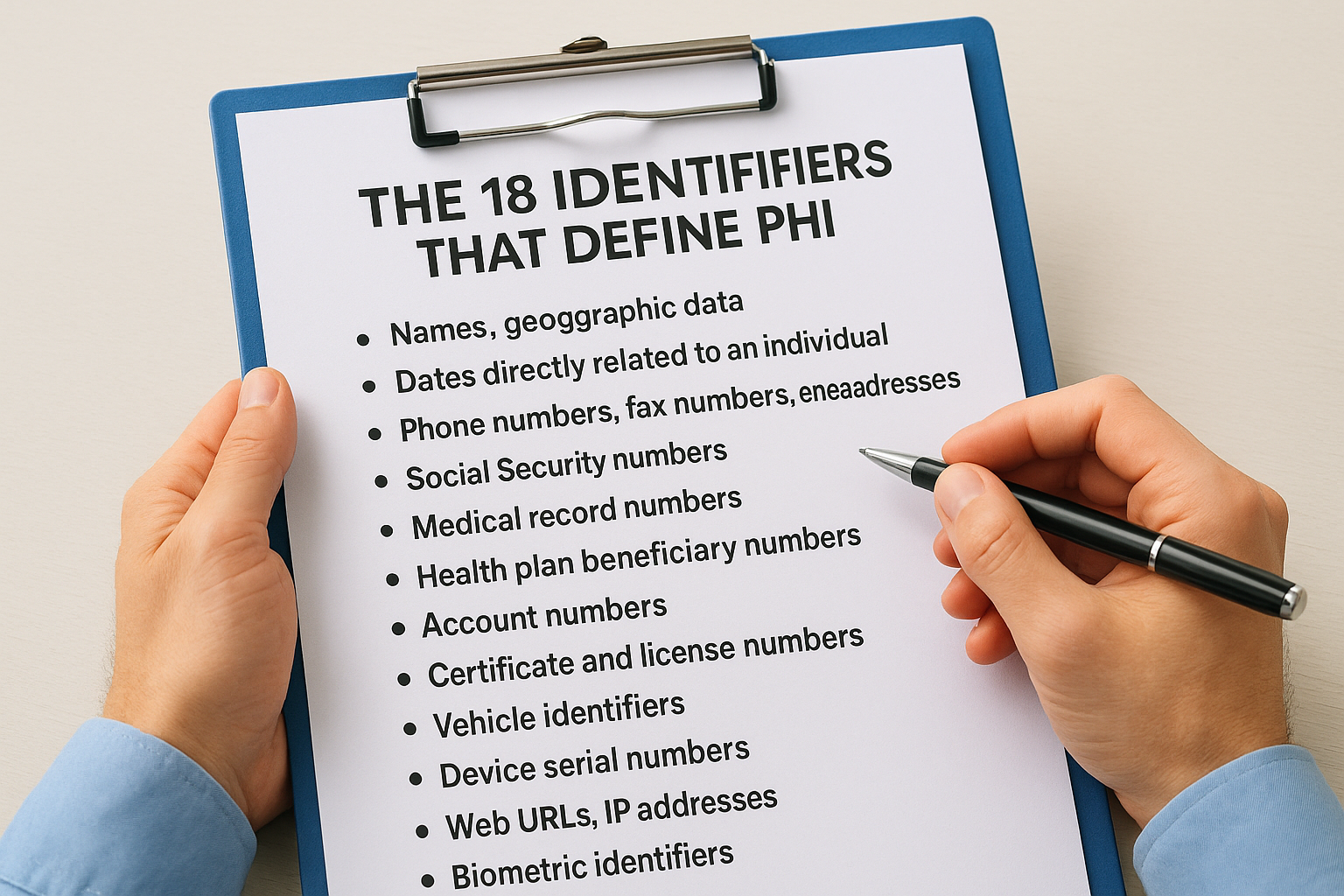
- Names, geographic data smaller than a state, and dates directly related to an individual (birth dates, admission dates, discharge dates)
- Phone numbers, fax numbers, email addresses, and Social Security numbers
- Medical record numbers, health plan beneficiary numbers, and account numbers
- Certificate and license numbers, vehicle identifiers, and device serial numbers
- Web URLs, IP addresses, biometric identifiers like fingerprints, and full-face photographs
- Any other unique identifying number or code that could link back to an individual
Removing all 18 identifiers from a dataset and verifying that it cannot be re-identified is how you achieve the "safe harbor" de-identification standard under HIPAA.
Information that falls outside PHI
Not all health-related data qualifies as PHI, and understanding those boundaries saves your team from over-engineering access controls on data that does not require them. Employment records held by an employer in its role as an employer are not PHI, even when they contain health information gathered through a workplace wellness program. De-identified data that has had all 18 identifiers removed through an accepted method is also outside the rule's scope and can move more freely between systems.
Your application may also handle data generated by patients themselves through consumer devices or personal health apps. Because those sources are typically not covered entities, the information they generate does not automatically qualify as PHI, though it may fall under other applicable privacy laws depending on how your platform processes it.
When you can use or disclose PHI without authorization
The Privacy Rule does not require patient authorization for every use of PHI. It identifies specific situations where disclosing or using protected health information is either permitted or required without getting a signed release from the patient. Knowing these permitted pathways is a core part of any HIPAA Privacy Rule summary because they define the legal foundation for most health data exchanges that your application will actually facilitate.
Treatment, payment, and healthcare operations
The most frequently used permitted disclosure category covers treatment, payment, and healthcare operations, commonly abbreviated as TPO. Under this pathway, covered entities can share PHI without authorization whenever it serves one of these three purposes. Treatment includes sharing records between providers coordinating a patient's care. Payment covers billing workflows and claims processing. Healthcare operations includes quality assessments, staff training, and compliance audits.

This TPO exception is the legal basis for most EHR integrations, which means your application's core data flows almost certainly rely on it.
For software platforms that integrate with EHR systems, the TPO exception is not a loophole but a deliberately structured permission that reflects how healthcare actually functions. When your application pulls a patient's medication list to support a care coordination workflow, that access sits within the treatment purpose, provided the covered entity using your platform has a valid care relationship with that patient.
Other permitted disclosures without patient authorization
Beyond TPO, the rule identifies a set of specific public interest and policy purposes that allow PHI disclosure without authorization. These include reporting to public health authorities, disclosures required by law such as court orders, reporting abuse or neglect to government agencies, responses to law enforcement requests that meet specific legal criteria, and releases to avert serious threats to health or safety.
Covered entities can also disclose PHI to the individual it belongs to without requiring that person to authorize their own access. Workers' compensation programs, certain government benefit programs, and oversight activities by agencies like HHS also qualify as permitted disclosures. Each category carries its own specific conditions, and your platform should never treat these exceptions as blanket permissions. Every permitted disclosure still requires that you share only the minimum amount of PHI necessary to accomplish the stated purpose, which is a requirement we cover in the next section.
Minimum necessary standard and practical examples
The minimum necessary standard is one of the most operationally significant requirements in any HIPAA Privacy Rule summary. It states that covered entities and business associates must make reasonable efforts to limit PHI access to only what is actually needed to accomplish the intended purpose. This is not a vague guideline. It is a concrete obligation that shapes how you design access controls, structure API requests, and configure user permissions within your application.
What the minimum necessary standard requires
The standard applies to uses, disclosures, and requests for PHI, but it does not apply to disclosures made directly to the patient, disclosures made to HHS for compliance investigations, or disclosures required by law. For everything else, your organization needs documented policies that define what PHI each role or workflow actually needs, rather than granting broad access by default. Covered entities must identify categories of employees and the specific data each category can access, based on job function, not on convenience.
Granting staff access to entire patient records when their role only requires a specific data field is a direct violation of this standard, even if no unauthorized disclosure ever occurs.
Your policies also need to account for requests you make to other covered entities. When your application requests PHI from an EHR on behalf of a care workflow, that request should specify only the data fields the workflow requires. Pulling a full patient record when you only need a medication list fails the minimum necessary test.
Practical examples of applying the standard
Applying this standard in a real integration context comes down to specificity at every layer of your data architecture. A billing team member needs diagnosis codes and insurance identifiers but has no legitimate reason to access psychiatric notes. A scheduling coordinator needs appointment history and contact information but does not need lab results. Each of those access boundaries must be reflected in your system's role-based permissions, not just your written policy.
For application developers building on top of EHR APIs, this means scoping your OAuth token requests to the narrowest FHIR resource types your use case genuinely requires. If your application supports medication management, requesting access to the full patient record scope exceeds what the minimum necessary standard permits. Narrowing your data requests also reduces your risk surface and simplifies your compliance documentation when health systems audit your integration.
Patient rights under the HIPAA Privacy Rule
The Privacy Rule is not just a set of restrictions on how organizations handle data. It also grants patients specific, enforceable rights over their own health information. Any practical HIPAA Privacy Rule summary needs to cover these rights in detail because your application's workflows must support them, not just avoid violating them. Covered entities and their business associates are legally required to honor these rights within defined timeframes, and building that capability into your platform from the start is far easier than retrofitting it later.
The right to access and receive copies of records
Patients have the right to inspect and obtain copies of their PHI held in a covered entity's designated record set. This includes medical records, billing records, and any other records used to make decisions about the individual. You must provide access within 30 days of a request, with one possible 30-day extension if you notify the patient in writing. Covered entities can charge a reasonable, cost-based fee for copies, but they cannot deny access simply because the patient has an outstanding balance.

Denying a patient access to their own records because of an unpaid bill is a direct Privacy Rule violation, regardless of the amount owed.
There are narrow exceptions where you can withhold specific information, such as psychotherapy notes or information compiled for legal proceedings, but these exceptions are limited and must be documented carefully. Your system needs a clear, auditable process for receiving, tracking, and fulfilling access requests within the required window.
The right to amend, restrict, and receive an accounting
Patients can request amendments to their PHI if they believe information in their record is incorrect or incomplete. You are not required to accept every amendment request, but you must respond within 60 days and provide a written denial if you reject the request, along with the patient's right to submit a statement of disagreement.
Patients also have the right to request restrictions on certain uses and disclosures of their PHI, and to receive an accounting of disclosures made outside of treatment, payment, and operations over the prior six years. One specific restriction is absolute: if a patient pays out of pocket in full for a service and requests that the information not be shared with their health plan, you must honor that restriction without exception.
Compliance requirements organizations must implement
No HIPAA Privacy Rule summary is complete without covering the operational requirements that make all the restrictions and patient rights enforceable in practice. The rule does not just describe what you cannot do with PHI. It also specifies a concrete set of administrative and procedural obligations that your organization must put in place and maintain continuously, not just at the start of a compliance program.
Privacy policies, notice of privacy practices, and staff training
Your organization must develop and implement written privacy policies and procedures that accurately reflect how you actually handle PHI. These policies need to cover permitted uses, disclosure controls, patient rights procedures, and how your staff handles violations. A policy that sits in a shared folder and no one reads does not satisfy this requirement. The rule requires that you train every member of your workforce on your privacy policies as a condition of their employment, and you must document that training occurred.
Covered entities must also provide patients with a Notice of Privacy Practices (NPP), a written document that explains how the organization uses and discloses PHI, what patient rights exist under the rule, and how patients can file complaints. You must deliver this notice at the first point of service and make it available on your website if you maintain one. Patients do not need to sign the NPP to receive care, but you must document your good-faith effort to obtain their acknowledgment.
Skipping staff training or maintaining outdated privacy policies are among the most commonly cited deficiencies in HIPAA compliance investigations.
Administrative, technical, and physical safeguards
Beyond documentation, you must designate a Privacy Officer who is responsible for developing policies, receiving complaints, and ensuring ongoing compliance across the organization. This person does not need to be a full-time dedicated role in smaller organizations, but accountability must sit with a named individual. You also need a process for receiving, tracking, and resolving privacy complaints from patients and staff, with records retained for at least six years.
Your technical environment must support the policies you have written. That means access controls that enforce role-based permissions, audit logs that record who accessed PHI and when, and encryption that protects data in transit and at rest. Physical access controls for locations where PHI is stored or processed round out the safeguard layer. These requirements overlap with the HIPAA Security Rule, but the Privacy Rule independently mandates reasonable safeguards as part of its own compliance framework.
Enforcement, penalties, and how complaints work
Understanding enforcement is the part of any HIPAA Privacy Rule summary that often gets skipped until something goes wrong. The HHS Office for Civil Rights (OCR) is the primary agency responsible for investigating complaints and enforcing compliance with the Privacy Rule. OCR has broad authority to investigate covered entities and business associates, issue corrective action plans, and impose civil monetary penalties when violations are confirmed.
How OCR investigates violations
OCR receives complaints from patients, staff, and other parties, and it also conducts compliance reviews on its own initiative. When a complaint is filed, OCR first determines whether it has jurisdiction, meaning the complaint involves a covered entity or business associate and falls within the Privacy Rule's scope. If jurisdiction exists, OCR notifies the organization under review and begins gathering evidence.
Most investigations result in a resolution agreement rather than a financial penalty, but only when the organization demonstrates good faith and takes corrective action promptly.
Many cases close through voluntary compliance or technical assistance, where OCR provides guidance and the organization corrects the identified deficiency without formal action. When an organization fails to cooperate or the violation is severe, OCR escalates to civil monetary penalties.
Penalty tiers and what they apply to
The penalty structure uses four tiers based on culpability, and the amounts differ significantly depending on whether you knew about the violation or acted with willful neglect. The tiers range from situations where the covered entity did not know and could not have known about the violation, up to cases involving willful neglect that went uncorrected. Annual penalty caps per violation category reach up to $1.9 million, adjusted periodically for inflation. The Department of Justice handles criminal penalties separately for cases involving intentional misuse of PHI.
How patients file complaints
Patients who believe their Privacy Rule rights have been violated can file a complaint directly with OCR through the HHS website. Complaints must be filed within 180 days of when the patient knew or should have known about the violation, though OCR can waive that deadline for good cause. Your organization cannot retaliate against any individual for filing a complaint, and you must document your anti-retaliation policies in writing as part of your compliance program. Patients can also file complaints with your organization's designated Privacy Officer directly, which gives you an opportunity to resolve issues before they reach OCR.
Key takeaways
This hipaa privacy rule summary covers the core elements your organization needs to understand and act on. The rule applies to covered entities and their business associates, protects individually identifiable health information across 18 specific identifier categories, and permits certain disclosures for treatment, payment, and healthcare operations without patient authorization. Patients hold enforceable rights over their records, including access, amendment, and restriction requests, and your platform must support those rights within defined timeframes.
Every data integration you build that touches patient records carries compliance obligations under this rule. Getting compliant starts with understanding the requirements, but staying compliant in production requires infrastructure that enforces them at every layer. If your team is building EHR integrations and needs a HIPAA-compliant foundation that handles authorization, data scoping, and audit logging from day one, launch your SMART on FHIR app and see how SoFaaS manages the integration complexity for you.
The Future of Patient Logistics
Exploring the future of all things related to patient logistics, technology and how AI is going to re-shape the way we deliver care.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.