Zero Trust Principles: Pillars, Model, And Best Practices

Every API call that touches patient data is a potential attack surface. Every EHR connection, every OAuth token exchange, every data sync between systems, each one represents a decision point where access is either properly verified or blindly trusted. Zero trust principles exist because that blind trust has repeatedly proven to be a costly mistake, especially in healthcare, where a single breach can expose millions of protected health records and trigger regulatory consequences that sink companies.
Zero trust isn't a product you install. It's a security model built on a straightforward idea: never trust, always verify. No user, device, or application gets automatic access to anything, not even if it's sitting inside your network perimeter. Every request must be authenticated, authorized, and continuously validated. For teams building healthcare applications that connect to EHRs like Epic, Cerner, or Allscripts, these principles aren't theoretical. They're the foundation of compliant, secure integration.
This is exactly why we built SoFaaS with zero trust baked into the architecture. Our HIPAA-compliant, SOC 2 Type II certified platform handles OAuth authorization management, end-to-end encryption, and audit logging so that healthcare innovators can integrate with EHR systems without building security infrastructure from scratch. We think about access verification at every layer so you can focus on your application.
This article breaks down the core pillars of the zero trust model, walks through its guiding principles, and covers practical best practices you can apply, whether you're securing a healthcare integration pipeline or rethinking your organization's security posture from the ground up.
What zero trust means and what it is not
Zero trust is a security framework built on the assumption that no user, device, application, or network connection should be trusted by default, regardless of where it originates. The model was formally introduced by John Kindervag at Forrester Research in 2010 and has since become the standard approach for securing cloud infrastructure, distributed systems, and data-sensitive pipelines, including those in healthcare. The core premise is direct: trust must be earned through verified identity and policy, not assumed because a request comes from inside a known network segment.
The core definition: verify everything, every time
The phrase "never trust, always verify" captures the operating logic well. Under zero trust principles, every access request is treated as potentially hostile until the system authenticates it and authorizes it against defined policy. This applies equally to internal users and external ones. A developer on your internal network requesting patient data through an EHR API must pass the same verification checks as a request arriving from a completely external endpoint. Location inside the network perimeter grants nothing on its own.
If your security model grants automatic access to any resource based solely on network location, you are not operating under zero trust.
Continuous validation is what separates zero trust from traditional perimeter-based security. Verifying identity once at login is not sufficient. The system must re-evaluate trust signals throughout every session, including device health, user behavior patterns, access scope, and contextual risk signals. This ongoing verification is what gives zero trust its resilience against credential theft and lateral movement attacks.
What zero trust is not
Zero trust is not a single product or technology you can purchase and deploy. Vendors frequently market firewalls, identity platforms, and access gateways as "zero trust solutions," but no single tool delivers the full model. Zero trust is a strategy that spans identity management, device security, network segmentation, application-layer controls, and data protection working together under a unified policy framework.
Zero trust is also not equivalent to using a VPN. A VPN grants broad network access once a user authenticates, which directly contradicts zero trust's requirement of least-privilege access. A compromised VPN credential can expose an entire network segment. Zero trust architecture limits that damage by granting access only to the specific resources a verified user needs for a defined task.
Finally, zero trust is not a project you finish and move on from. Implementing zero trust is a continuous commitment that requires ongoing monitoring, policy refinement, and adaptation as your infrastructure scales and your threat environment shifts. Treating it as a one-time deployment rather than an operational posture is where most organizations create exploitable gaps.
Why zero trust matters in modern healthcare IT
Healthcare is one of the most frequently targeted industries for cyberattacks. Patient records contain a dense concentration of personally identifiable information, financial data, and medical history, making them significantly more valuable on criminal markets than stolen credit card numbers. According to IBM's Cost of a Data Breach Report, healthcare breaches carry the highest average cost of any industry, consistently exceeding $10 million per incident. When your application connects to EHR systems and exchanges protected health information, every integration point becomes a potential entry path for attackers if access controls are not built on verified trust from day one.
The compliance pressure is real and growing
HIPAA and the HITECH Act require covered entities and business associates to implement technical safeguards that restrict access to protected health information strictly to authorized users and systems. Zero trust architecture maps directly onto these requirements by enforcing least-privilege access, continuous session validation, and detailed audit logging across every system that handles patient data. Failing to meet these mandates doesn't just create security risk; it creates direct legal and financial exposure that can end a company's ability to operate in healthcare. Applying zero trust principles to your EHR integration stack puts you in a far stronger position during a compliance audit because you can demonstrate that access was verified, not assumed.
Healthcare organizations that enforce zero trust controls on their integrations are better positioned to demonstrate HIPAA compliance because every access event is authenticated, logged, and tied to a verified identity.
EHR integrations create specific attack surfaces
Connecting your application to systems like Epic or Cerner introduces OAuth token flows, API endpoints, and data synchronization pipelines that each require their own layer of access controls. Without a zero trust approach, a single compromised token or misconfigured API permission can expose patient data well beyond any individual user's intended scope. Short-lived tokens, role-based permissions, and continuous session monitoring reduce the blast radius when any one credential is compromised. Your integration layer is a direct extension of your security perimeter and needs to be treated with the same rigor as your core application infrastructure.
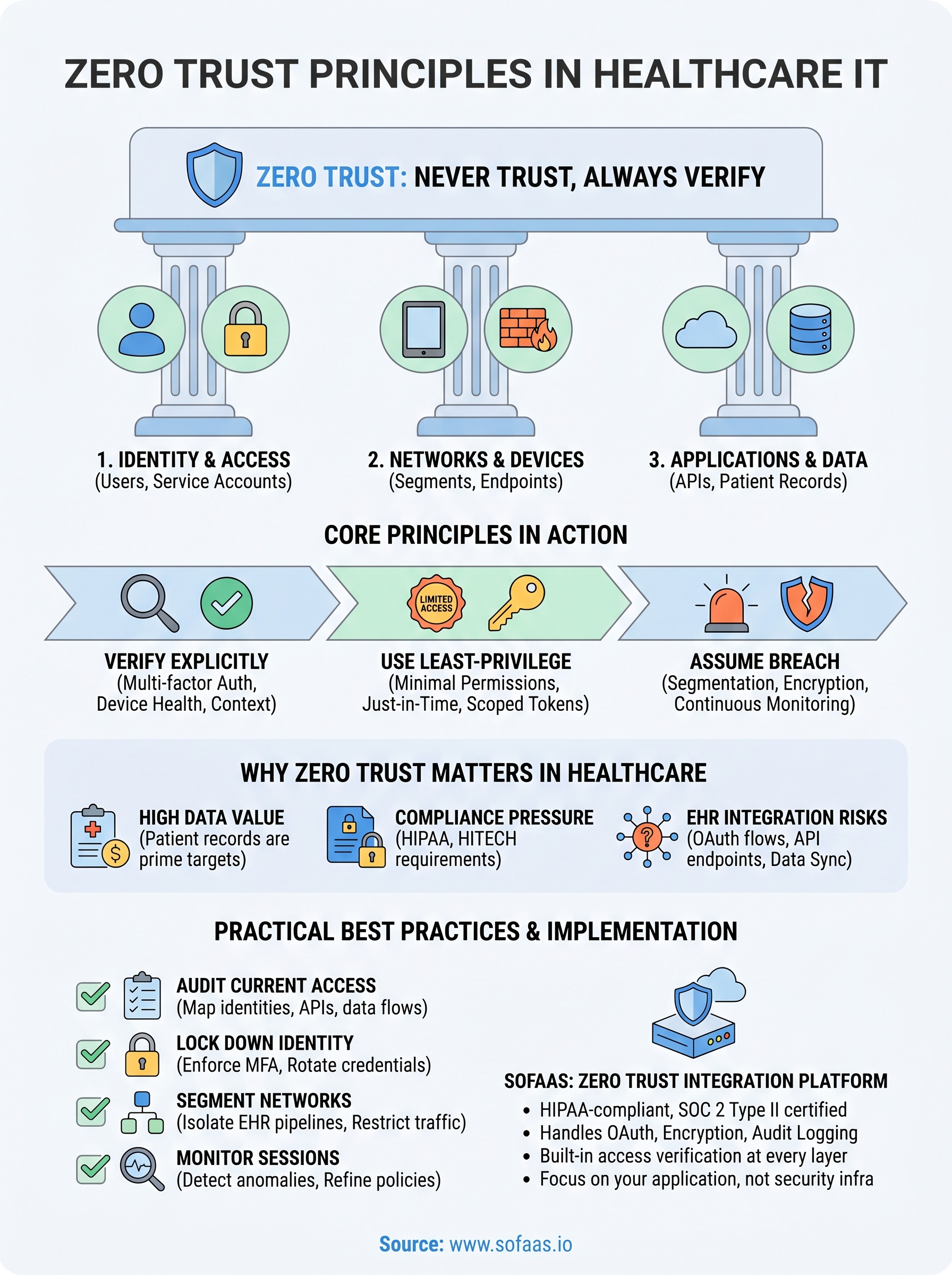
The three core zero trust principles
The zero trust model is grounded in three foundational principles that define how every access decision should work. These aren't abstract guidelines. They're operational rules that shape how your systems authenticate requests, grant permissions, and respond when something goes wrong. Understanding all three gives you the foundation to evaluate any security architecture honestly.

Verify explicitly
Explicit verification means your systems authenticate and authorize every request based on all available signals, not just a username and password. Those signals include device health, location, IP reputation, user behavior patterns, and the sensitivity of the resource being accessed. A request that looks legitimate but originates from an unmanaged device flagged for suspicious activity should trigger additional scrutiny or be denied outright. Nothing passes through based on assumed trust alone.
Use least-privilege access
Every user, service account, and application should receive only the minimum permissions required to complete a specific task, nothing more. In practice, this means scoping OAuth tokens to exact FHIR resource types, limiting API permissions by role, and applying just-in-time access controls that expire once a session ends. The goal is to contain the damage any single compromised credential can cause. If an attacker steals a token with broad permissions, they can move laterally. If that token was scoped tightly, the blast radius stays small.
Least-privilege access is where most healthcare integration security breaks down: overly broad API permissions create exposure that no amount of perimeter defense can contain.
Assume breach
Assume breach is the most important mindset shift in zero trust principles. You design your systems as if attackers are already inside. That means segmenting network access, encrypting data in transit and at rest, enforcing continuous session validation, and maintaining detailed audit logs so you can detect and respond to anomalous behavior quickly. Rather than hoping your perimeter holds, you build controls that limit what any attacker can reach once they're in.
The five pillars of zero trust and what to secure
Zero trust principles organize security across five distinct pillars: identity, devices, networks, applications and workloads, and data. Each pillar represents a category of resources that requires its own verification and access controls. Together, they define what you must secure and how those controls interact to form a complete zero trust architecture.

| Pillar | What you secure |
|---|---|
| Identity | Users, service accounts, and roles |
| Devices | Endpoints, managed and unmanaged |
| Networks | Segments, traffic flows, micro-perimeters |
| Applications & Workloads | APIs, services, cloud workloads |
| Data | Patient records, tokens, sensitive payloads |
Identity and devices
Identity is the new perimeter in zero trust. Every user and service account must be verified continuously using multi-factor authentication and behavioral signals, not just at login. Your service accounts and API credentials are identities too, and they require the same scrutiny as human users.
Devices form the second pillar because an authenticated user on a compromised endpoint is still a threat. Your zero trust controls should check device health, patch status, and compliance posture before granting access. Unmanaged or out-of-compliance devices should receive limited or no access regardless of user credentials.
Networks, applications, and data
Network segmentation limits lateral movement by dividing your infrastructure into micro-perimeters, so a compromised segment cannot freely access adjacent resources. For healthcare integrations, this means your EHR connection pipeline operates in an isolated segment with tightly controlled inbound and outbound traffic rules.
Data is the ultimate target in every healthcare breach, which makes it the most critical pillar to protect with encryption, classification, and access scoping at the resource level.
Applications and data complete the model by enforcing controls at the workload and resource layer. Your APIs should validate tokens against exact permission scopes, and patient data should be classified and encrypted both in transit and at rest so that access at the application layer never exposes more than a specific request requires.
How to implement zero trust in a real environment
Applying zero trust principles to a live environment requires you to move methodically through each security layer rather than attempting a full overhaul at once. Start by auditing what you currently have: map every identity, every access path, every API connection, and every data flow that touches sensitive resources. That inventory becomes your baseline for knowing what needs controls and where your largest exposures sit right now.
Lock down identity and access first
Identity controls are the highest-impact starting point because they directly address how every user and service account gains access to your systems. Enforce multi-factor authentication across all accounts, rotate credentials on a defined schedule, and assign role-based permissions that reflect the minimum access each identity actually needs. For healthcare API integrations, that means scoping OAuth tokens to specific FHIR resource types and revoking them automatically when a session ends rather than allowing long-lived credentials to persist.
Implementing MFA and scoped token access alone eliminates a significant portion of the credential-based attack vectors that cause most healthcare data breaches.
Segment your network and enforce API-layer controls
Network segmentation limits what attackers can reach if any single component is compromised. Divide your infrastructure so your EHR integration pipeline runs in an isolated segment with tightly restricted traffic rules. At the API layer, validate every token against its exact permission scope on each request. Do not rely on perimeter firewalls alone to protect data flowing between your application and EHR systems like Epic or Cerner.
Monitor sessions and refine policies continuously
Zero trust requires you to treat implementation as an ongoing operational process, not a finished project. Set up continuous session monitoring that flags anomalous behavior, unusual access patterns, or requests from unhealthy devices in real time. Review your access logs regularly and tighten policies based on what you observe. Your threat environment changes as your infrastructure scales, and your zero trust controls need to adapt at the same pace.
Next steps
Zero trust principles give you a clear framework for making every access decision deliberate and verifiable rather than assumed. You now have the core model, the five pillars, and a practical starting path for applying these controls to your own environment. The gap between understanding zero trust and operating it closes when you start auditing your current access paths, tightening identity controls, and treating every integration point as a potential attack surface that requires explicit verification.
For healthcare teams building on EHR integrations, that work gets significantly harder when you're managing OAuth flows, HIPAA compliance, and API-layer security from scratch. SoFaaS handles the security infrastructure your integration depends on so you can move from development to production without building compliance controls yourself. If you're ready to connect your healthcare application to Epic, Cerner, or Allscripts with HIPAA-compliant, zero trust security built in from day one, launch your SMART on FHIR integration with SoFaaS.
The Future of Patient Logistics
Exploring the future of all things related to patient logistics, technology and how AI is going to re-shape the way we deliver care.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.