HIPAA Security Rule Requirements: Safeguards Explained

Every organization that handles electronic protected health information (ePHI) faces the same regulatory baseline: the HIPAA Security Rule requirements. These requirements aren't suggestions or best practices, they're federal mandates backed by enforcement actions, financial penalties, and reputational consequences. Yet many healthcare technology teams still struggle to translate the rule's language into concrete, implementable controls across their systems and workflows.
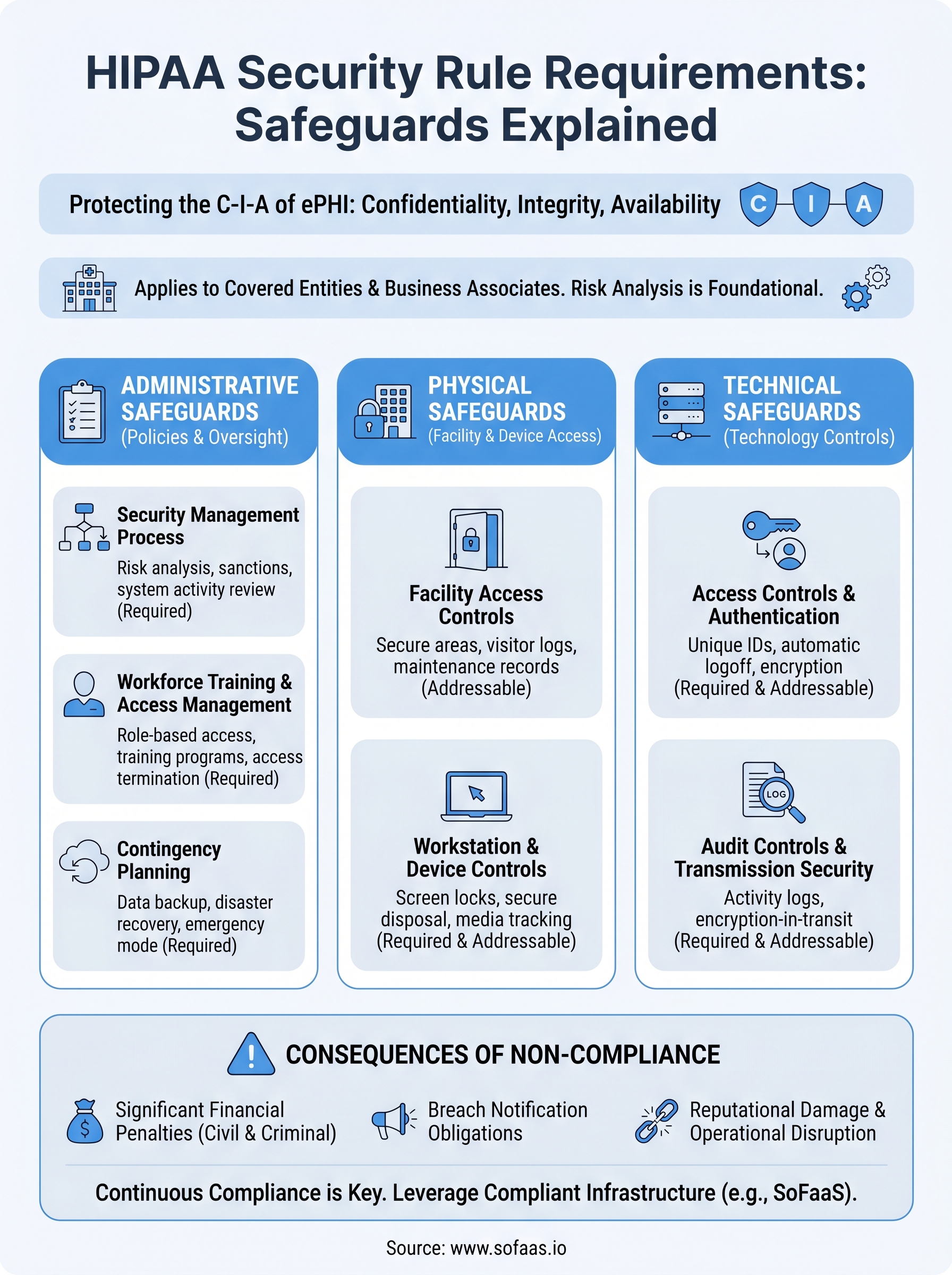
The Security Rule breaks down into three categories of safeguards, administrative, physical, and technical, each with required and addressable implementation specifications. Understanding what falls into each category, and what "addressable" actually means (hint: it doesn't mean optional), is critical for anyone building or operating technology that touches patient data. This applies whether you're a covered entity, a business associate, or a software vendor integrating with EHR systems.
This is exactly why platforms like SoFaaS exist. Built by VectorCare, SoFaaS handles SMART on FHIR integrations with HIPAA-compliant infrastructure and SOC 2 Type II controls baked in, so development teams can connect to EHRs like Epic and Cerner without engineering their own compliance and security stack from the ground up.
In this article, we'll walk through each safeguard category in the HIPAA Security Rule, explain what the specific standards require, and clarify where organizations most commonly fall short. Whether you're preparing for an audit or evaluating your integration architecture, this breakdown will give you a practical understanding of what compliance actually demands.
Why HIPAA security rule requirements matter
The HIPAA Security Rule isn't a compliance checkbox you satisfy once and move on from. It's a living set of standards that the Department of Health and Human Services (HHS) enforces actively through its Office for Civil Rights (OCR). When organizations treat security requirements as secondary to product development, they expose themselves to consequences that go far beyond a single fine. Understanding why these requirements exist and what happens when they're ignored gives you the context to take them seriously from the earliest stages of your architecture.
The financial cost of non-compliance
Financial penalties under HIPAA operate on a tiered structure tied directly to the level of culpability. Civil monetary penalties can reach between $100 and $50,000 per violation, and the annual cap for violations within a single category sits at $1.9 million. When OCR investigates a breach and finds systemic failures across multiple safeguard categories, the penalties compound quickly. A 2023 settlement with Lafourche Medical Group reached $480,000 after a phishing attack exposed data for roughly 34,000 patients, and the investigation revealed the organization had never conducted a formal risk analysis.
Organizations that skip foundational HIPAA security rule requirements often face compounding penalties because a single incident surfaces multiple missing controls at once.
Beyond civil penalties, the Department of Justice handles criminal referrals for willful neglect or deliberate misuse of patient data. Criminal convictions can carry prison sentences of up to 10 years for the most serious violations. For any software vendor or integration platform operating in healthcare, those outcomes aren't theoretical risks. They're documented outcomes that have ended businesses and careers.
Breach notification obligations and their ripple effects
A security failure doesn't stay contained to your internal systems. Under HIPAA's Breach Notification Rule, you must notify affected individuals, HHS, and in many cases the media within 60 days of discovering a breach involving unsecured ePHI. That notification requirement triggers an automatic OCR investigation whenever a breach affects 500 or more individuals in a single state or jurisdiction. Your legal, communications, and engineering teams all get pulled into the response at the same time, while your core product work stops.
The operational disruption that follows a breach typically costs more than the penalty itself. Forensic investigation fees, legal counsel, notification logistics, and remediation of the underlying vulnerability add up quickly, often into the millions. Patient trust, once broken, is difficult to rebuild, and health tech companies that experience public breaches regularly report lasting damage to both customer retention and new business development.
Why technical integrations carry particular risk
Healthcare integrations, especially those connecting applications to EHR systems via SMART on FHIR, sit at the intersection of complex data flows, patient authorization, and multi-system architecture. Each connection point in that stack represents a potential exposure surface. If your integration layer lacks proper encryption, audit logging, or access controls, a breach at that layer can affect every patient whose data moves through it, regardless of how secure the EHR itself might be.
Managing these risks effectively requires deep expertise in both HIPAA security rule requirements and the specific technical configurations of each EHR system you connect to. That's a significant burden for any team whose core focus is building healthcare applications rather than maintaining integration infrastructure.
Who must comply and what counts as ePHI
Before you can apply the HIPAA Security Rule requirements to your organization, you need to know whether they apply to you at all, and what specific data they govern. The scope of the rule extends further than most teams initially assume, and misidentifying either your compliance category or your data type creates gaps that can surface during audits or breach investigations.
Covered entities and business associates
The Security Rule applies directly to covered entities, which include health plans, healthcare clearinghouses, and healthcare providers that transmit health information electronically. But it also applies to business associates, meaning any organization that creates, receives, maintains, or transmits ePHI on behalf of a covered entity. If you build a healthcare application, operate an EHR integration platform, or provide cloud infrastructure to healthcare clients, you almost certainly qualify as a business associate under this definition.
Subcontractors of business associates carry the same HIPAA obligations as the business associate itself, which means the compliance chain extends through your entire vendor stack.
Your compliance obligations as a business associate must be formalized through a Business Associate Agreement (BAA) signed with each covered entity you work with. Without a valid BAA in place, you're operating outside the bounds of HIPAA's permissible data sharing framework, regardless of how strong your technical controls actually are.
What qualifies as ePHI
Protected health information (PHI) covers any individually identifiable health information that relates to a person's past, present, or future health condition, healthcare treatment, or payment for care. The "electronic" designation simply means that information exists in or moves through an electronic format, including data stored in databases, transmitted over APIs, or processed in cloud systems. When your application pulls patient records from an EHR via SMART on FHIR, every data element returned in that exchange is ePHI.
The category is broader than most developers expect. Demographic data like names, addresses, dates of birth, and Social Security numbers all qualify as ePHI when they're linked to health information. Even device identifiers or IP addresses can fall under PHI if they connect a specific individual to a health record. Understanding these boundaries precisely shapes every technical and administrative decision you'll make to stay compliant.
General requirements and key security concepts
The Security Rule sets a baseline obligation before you even get to the specific safeguard categories: you must protect the confidentiality, integrity, and availability of all ePHI your organization creates, receives, maintains, or transmits. That three-part standard shapes every decision you'll make when implementing hipaa security rule requirements across your infrastructure, policies, and workflows.
Required vs. addressable implementation specifications
Each standard within the Security Rule carries implementation specifications, and those specifications are labeled either "required" or "addressable." Required specifications have no flexibility. You must implement them exactly as written. Addressable specifications give you more latitude, but that doesn't mean you can skip them. If an addressable specification is reasonable and appropriate for your environment, you must implement it. If you determine it isn't, you must document your reasoning and implement an equivalent alternative measure.
Many organizations misread "addressable" as optional and leave gaps in their controls that become critical findings during OCR audits.
This distinction matters because auditors and investigators will ask you to demonstrate that every addressable specification was evaluated deliberately. Undocumented decisions carry the same risk as missing controls, because you can't prove the evaluation happened if nothing is written down.
The risk analysis mandate
Before you can implement any safeguard correctly, you need to know what threats your ePHI actually faces. The Security Rule requires you to conduct an accurate and thorough assessment of potential risks and vulnerabilities to the ePHI your organization holds. This risk analysis isn't a one-time task. You must review and update it whenever your environment changes, such as when you add a new EHR integration, move infrastructure to a new cloud provider, or onboard a new business associate.
Your risk analysis also determines the scope and priority of your security measures. If you haven't mapped where ePHI lives and flows through your systems, you can't know whether your administrative, physical, and technical safeguards actually cover it. A gap in your risk analysis almost always becomes a gap in your controls, and OCR settlements consistently cite the absence of a completed risk analysis as a primary finding. Organizations that build integrations connecting to EHR systems via APIs need to include every data flow, authentication exchange, and storage layer in that analysis from the start.
Administrative safeguards you must implement
Administrative safeguards are the policies, procedures, and oversight structures that govern how your organization manages ePHI access and risk. The HIPAA Security Rule requirements place administrative safeguards first in their structure because no technical control works correctly without the organizational foundation behind it. If your policies don't define who can access what data, your access controls have no direction. If your workforce hasn't been trained, your technical safeguards get bypassed through human error before they ever do their job.

Security management process
The security management process standard requires you to implement policies and procedures to prevent, detect, contain, and correct security violations. This includes your risk analysis, a formal risk management plan that addresses identified vulnerabilities, a sanctions policy for workforce members who violate your security policies, and an information system activity review that monitors audit logs and access records on a regular basis. These four implementation specifications are all required, meaning you can't substitute alternatives for any of them.
Skipping the sanctions policy is a common gap that signals to auditors your workforce accountability structure is incomplete, even if your technical controls look solid.
Workforce training and access management
Your workforce is both your most valuable resource and your highest-risk exposure point when it comes to ePHI. The Security Rule requires you to implement security awareness and training programs for all workforce members, including management. Training isn't a one-time onboarding task. You need to update it when threats change, when your systems change, or when a security incident reveals a gap in understanding.
Access management runs alongside training. You must establish procedures for granting ePHI access based strictly on job function, terminating access when someone leaves or changes roles, and reviewing access privileges on a defined schedule. Organizations that let access accumulate over time, where former employees or role-changers retain permissions they no longer need, create exposure points that surface repeatedly in breach investigations.
Contingency planning
Your contingency plan addresses what happens when systems fail or ePHI becomes unavailable. Required specifications include a data backup plan, a disaster recovery plan, and an emergency mode operation plan that keeps critical processes running during outages. You must also test and revise those plans on a defined schedule, because an untested recovery plan provides far less real protection than it appears to on paper.
Physical safeguards you must implement
Physical safeguards govern how your organization controls access to the facilities, workstations, and devices that store or process ePHI. The HIPAA Security Rule requirements treat physical access as a distinct and non-negotiable control layer, separate from your technical systems. A breach doesn't require a sophisticated cyberattack. An unlocked server room, an unattended workstation, or a stolen laptop can expose patient data just as effectively.

Facility access controls
Your facility access controls determine who can physically enter spaces where ePHI systems are located, and under what circumstances. You must implement contingency operations procedures that allow authorized personnel to access facilities during emergencies, alongside a facility security plan that prevents unauthorized physical access. You also need documented procedures for controlling access during normal operations, such as visitor management and badge access systems, and a record of hardware repairs or modifications to components that handle ePHI.
Organizations that rely on informal access policies for server rooms and data closets often discover during audits that they have no documentation trail to demonstrate who accessed what and when.
These controls apply whether your infrastructure sits in your own office or in a third-party data center. If you colocate servers or use a managed hosting environment, your vendor's physical security posture directly affects your compliance standing, which is why your risk analysis and business associate agreements need to address physical security explicitly.
Workstation and device controls
Workstations and mobile devices are where ePHI most frequently moves outside controlled environments. You must implement workstation use policies that define appropriate functions and the physical surroundings for each device accessing ePHI. Screens should face away from public view, and sessions should lock automatically after a defined period of inactivity. These specifications are required, not addressable.
Device and media controls cover the movement, reuse, and disposal of hardware that contains ePHI, including hard drives, USB devices, and portable media. You must track hardware assets, ensure data is properly purged before devices are reused or decommissioned, and maintain records of equipment movement. For teams running healthcare integrations across distributed environments, this means including every endpoint that receives or caches patient data from your API connections in your device inventory and disposal procedures.
Technical safeguards you must implement
Technical safeguards are the technology-based controls you use to protect ePHI as it's stored, processed, and transmitted across your systems. The HIPAA Security Rule requirements define four technical safeguard standards, and each one targets a specific point where patient data is vulnerable: who accesses it, what happens to it in transit, how changes are detected, and whether the records of access are preserved. Getting these controls right requires you to understand not just the standards themselves, but how they apply to every layer of your architecture, including API connections, cloud storage, and EHR integration pipelines.

Access controls and authentication
Your access controls determine which users and systems can reach ePHI and under what conditions. Required specifications include unique user identification, so every individual accessing your systems does so under a distinct identifier that ties activity to a specific person. You must also implement emergency access procedures that allow authorized personnel to retrieve ePHI when normal authentication methods are unavailable. Two addressable specifications round out this standard: automatic logoff after a period of inactivity and encryption and decryption controls for stored ePHI.
Shared login credentials undermine your entire audit trail because you can no longer attribute access events to a specific individual when an incident occurs.
Authentication strength directly affects your access control posture. Multi-factor authentication is not explicitly named in the Security Rule text, but your risk analysis will almost certainly identify it as a reasonable and appropriate measure given the current threat landscape, which means you need to document a deliberate decision about it either way.
Audit controls and transmission security
Audit controls require you to implement hardware, software, and procedural mechanisms that record and examine activity in systems containing ePHI. You must capture access logs, failed login attempts, data export events, and administrative changes across every system that touches patient data, including your integration middleware and API layers.
Transmission security protects ePHI moving across any network, internal or external. You must guard against unauthorized access during transmission, and the addressable specification calls for encryption whenever it's reasonable and appropriate, which covers virtually every modern network scenario. For teams running SMART on FHIR integrations, this means enforcing TLS across every API call that carries patient data between your application and connected EHR systems.
How to implement HIPAA security rule requirements
Turning the HIPAA security rule requirements into working controls starts with a structured implementation sequence, not a checklist you hand off to a single team. The most effective approach treats implementation as a cross-functional project that ties your risk analysis output directly to specific safeguard decisions across administrative, physical, and technical layers.
Start with your risk analysis and gap assessment
Your risk analysis is the map that tells you where ePHI actually lives and which safeguard controls you're currently missing. Before you write a single policy or configure a single access control, document every system, workflow, and integration that creates, receives, stores, or transmits ePHI. For teams running EHR integrations, this includes every API endpoint, authentication exchange, and data cache in your connection stack.
A thorough gap assessment run against each safeguard category gives you a prioritized remediation list rather than an overwhelming inventory with no clear starting point.
Once your gaps are mapped, assign explicit owners and realistic remediation timelines to each item. Unowned gaps stay open indefinitely, and OCR investigators will ask you to demonstrate not just that controls exist today, but that you identified and addressed gaps deliberately.
Build policies before you configure systems
Technical controls fail when the policies behind them are missing or vague. Before you configure access controls, audit logging, or encryption settings, document the policies that define how those controls should work. Your workforce access policy needs to specify who can access ePHI, under what conditions, and what the consequences are for violations.
Policies also give your technical team clear requirements to implement against. A well-written data transmission policy tells your engineers exactly which encryption standards apply to API traffic carrying patient data. Without that policy layer, technical teams make inconsistent decisions that leave uneven coverage across your systems.
Test, document, and revise on a defined schedule
Implementation isn't a one-time event. You need to test your controls regularly, verify they still address the risks your analysis identified, and update both policies and technical configurations whenever your environment changes. Document every test cycle, every finding, and every remediation action. That documentation trail is what demonstrates to auditors that your compliance program runs continuously, not just in the weeks before a scheduled review.
A simple way to stay compliant over time
Meeting hipaa security rule requirements is not a project you finish and archive. Every new EHR connection, cloud migration, or workflow change reopens your risk surface and demands a fresh review of your safeguards. The organizations that stay compliant are the ones that treat compliance as an ongoing operational discipline rather than a periodic scramble before an audit.
Building that discipline gets significantly easier when your integration infrastructure handles the hardest technical controls for you. If your EHR connections run on a platform that provides built-in HIPAA-compliant infrastructure, SOC 2 Type II controls, and automated audit logging, your team can stay focused on your application rather than re-engineering your compliance stack every time requirements or systems change.
That's exactly what SoFaaS delivers. Connect your healthcare application to EHRs with compliant SMART on FHIR infrastructure and stop building security and compliance controls from scratch.
The Future of Patient Logistics
Exploring the future of all things related to patient logistics, technology and how AI is going to re-shape the way we deliver care.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.